Request Medical Records Wellstar Health System
Get and sign wellstar medical release form (optional) zip code primary contact number wellstar authorization for the release of protected health information if we cannot reach you at the telephone number listed above, wellstar may contact you (including leaving messages) regarding appointments or normal lab results at the following number(s): business number cell phone number other phone number i authorize the wellstar medical group to disclose protected health. To obtain a copy of a wellstar medical record, we require a written request and properly executed patient authorization for disclosure of protected health information. this can be mailed to health information management, release of information services, at the address of the appropriate wellstar hospital. Keep to these simple instructions to get wellstar patient authorization for use and disclosure of protected health information completely ready for submitting: select the sample you want in the library of templates. open the form in the online editor. read the instructions to discover which information you need to include.
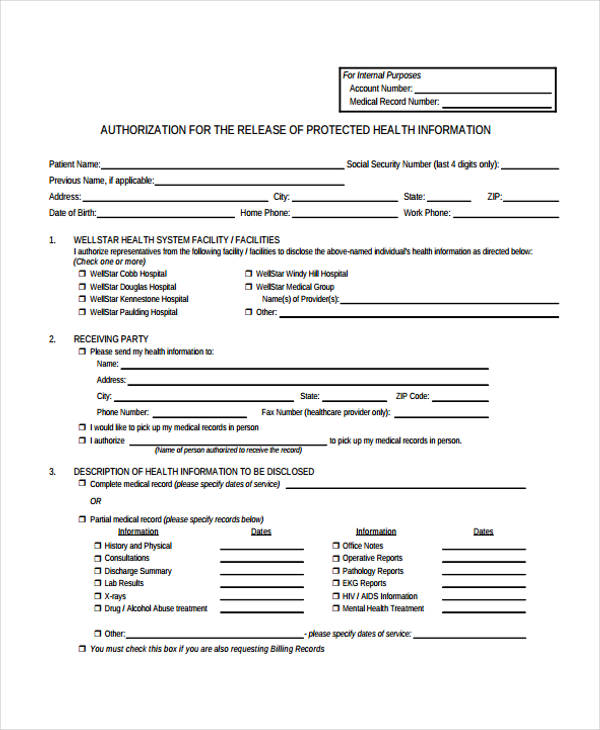
Authorization For The Release Of Protected Health Information
Provision of health care by wellstar is solely for the purpose of creating phi for disclosure to a third party legally authorized to receive such information. i understand that i will be given a copy of this authorization. signature/date:(date authorization signed by patient or legal guardian/personal representative) _____. Instructions for completing the authorization for release of protected health information (phi) fill out the form completely. the authorization is not valid unless it is filled out completely. section 1. member information to be released. include the following information about the member whose protected information is being disclosed: 1. Complete wellstar authorization for the release of protected health information 2020 online with us legal forms. easily fill out pdf blank, edit, and sign them. save or instantly send your ready documents.
Medical Records Release Request Wellstar Health System
Subject to the federal privacy regulations, my health information disclosed pursuant to this authorization may no longer be protected by the federal privacy regulations. 10. release and waiver. if the health information that i have requested wellstar health system to disclose contains any privileged psychiatric or psychological information. Wellstar~ ~-¥ medicalgroup. patient authorization for use and disclosure of protected health information. the information on this form. is. used tofacilitate our communications to you as we strive to provide you with excellent service. the provision ofthis information. is. optional. patient information (pleas e print clearly) : last name. first nam e. March 3, 2021 /prnewswire/ -wellstar health system additional information about the business combination and where to find it this press release contains forward-looking statements that. How to accomplish a wellstar patient authorization for use and disclosure of protected health information 0 on the web: on the web site with all the document, just click begin immediately along with complete to the manager. use the particular clues in order to submit the kind of job areas. type in your own info and phone info.
Wellstar Medical Release Form Fill Out And Sign
Authorizationfor the release of protected health information page 2 5. description of health information to be disclosed: complete medical record / health information (please specify dates of service): abstract of my health information (information needed for continuity of care: includes physician notes, emergency room records, test results,. Authorization for release of protected health information (phi) authorization to prescribe add medication request for religious exemption to immunization advance directives to register and request the wegmans prescription medication delivery service. The detroit land bank authority and the city's demolition department wasted time, resources and taxpayer dollars to determine if topsoil used by a now-banned demolition contractor was safe, an investi. Authorization for the release of protected health information all requests for medical records must be fully completed and dated on or after the date of discharge to be processed. after the properly executed authorization has been received, our team will review for all required elements and processes in accordance with federal and state laws governing you privacy and medical records.
Ws0464 / item 71432 original: wellstar / copy: patient rev. 07/22/03 authorization: “general” use & disclosure of protected health information (phi) wellstar location: (please 5 the applicable facility below) kennestone hospital windy hill hospital homecare cobb hospital paulding hospital hospice physician’s group:_____. Authorization for the release of wellstar authorization for the release of protected health information protected health information page 2 5. description of health information to be disclosed: complete medical record / health information (please specify dates of service): abstract of my health information (information needed for continuity of care: includes physician notes, emergency room records, test results,. Created date: 3/15/2013 12:39:49 pm.
Wellstar medical records. fill out, securely sign, print or email your medical release forms wellstar health system wellstar instantly with signnow. the most secure digital platform to get legally binding, electronically signed documents in just a few seconds. available for pc, ios and android. start a free trial now to save yourself time and money!. Health system for internal purposes account number: medical record number: authorization for the release of protected health information patient name: previous name, if applicable: address: date of birth: social security number (last 4 digits only): city: state: zip: home phone: work phone: 1. wellstar health system facility / facilities.
Place an electronic digital signature on your wellstar patient authorization for use and disclosure of protected health information 0 with the aid of signal instrument. when the shape is finished, media accomplished. send the set file through e mail or perhaps facsimile, art print against each other or perhaps save the your own system. Wellstar authorization for the release of protected health information 2020 4. 8 satisfied (53 votes) wellstar authorization for the release of protected health information 2018 wellstar authorization for the release of protected health information 2012-05 4. 4 satisfied (573 votes) related to wellstar records request. I understand that wellstar cannot require me to sign this authorization as a condition to treatment unless the provision of healthcare by wellstar is solely for the purpose of creating phi for disclosure to a third party legally authorized to receive such information. i understand that i will be given a copy of this authorization upon my signature.
All billing/account information authorization statement: i understand that protected health information (phi) used or disclosed pursuant to this wellstar authorization for the release of protected health information authorization may be subject to re-disclosure by the recipient and no longer protected by federal or state law. i understand that i have the right to revoke this authorization at any time. The person or organization sent or transporting the disclosed information under this authorization may disclose information again. it may not be possible to ensure your right to the protection of the privacy of this information once nextcare releases/discloses it to another party.


Federal health officials and an independent oversight board late monday accused astrazeneca of presenting the world with potentially misleading information about the effectiveness of the company's covid-19 vaccine,. Subject to the federal privacy regulations, my health information disclosed pursuant to this authorization may no longer be protected by the federal privacy regulations. 10. release and waiver if the health information that i have requested wellstar health system to disclose contains any privileged psychiatric or psychological information. Authorization for release of protected health information. i, wellstar authorization for the release of protected health information (name of patient) hereby authorize (name of person or facility which has information) to. release the following health information: to: (name and title or facility name to receive health information) (street address, city, state, zip code).
